Jaisson Maxime, Paris Marion, Salmi Ouassim
Abstract
In the case of a full mouth rehabilitation, the practitioner faces many challenges and needs to master crucial steps such as evaluating the patient and his needs as well as offering an adapted treatment.
How can digital tools help the practitioner in these challenges? And how to transfer all the digital data to the dental technician to work efficiently and without losing information? This clinical case illustrates how digital tools and especially MODJAW™ Tech in Motion™ allows the practitioner to work efficiently in a digital workflow, for the benefit of the patient.
Introduction
Digital dentistry is accelerating with the improvement and use of computer-aided design and computer aided manufacturing (CAD/CAM) in daily dental practice.1 In the case of a full mouth rehabilitation, many techniques and associated therapies are necessary, making it a real challenge for both the practitioner and the dental technician. These treatments require the establishment of a prosthetic project that will serve as a guide from the implant surgery to the final prosthesis.
The main objective of a full mouth rehabilitation is to restore the dentition by establishing new occlusal architecture and forms, at a correct vertical dimension while maintaining the health and harmony of the entire stomatognathic system.2,3 From this perspective, MODJAW™️ Tech in Motion™️ device completes the digital workflow by recording the functional envelop of a patient and helping in the predictability of a treatment plan, especially in the case of an immediate loading. It helps to overcome three main challenges encountered in full rehabilitations. The first challenge is to validate a therapeutic mandibular position, and to transfer it to the laboratory. The second challenge is to respect the occlusal and esthetic plane. The design of the occlusal anatomy respecting the patient’s specific movements and envelop of function (functional area) can be seen as the third challenge.4
The description of a situation of extraction- immediate implant placement will be used here as a support to the application of these new digital tools. The consultation is driven by the wish to regain a harmonious and pleasant smile, as well as masticatory efficiency (Figs. 1-3).

The MODJAW™️ System
MODJAW Tech in Motion is a Class I medical device composed of hardware and software based on the combination of 3D technology (3D models from intra-oral scanners) and motion capture techniques (Figs. 4 & 5). A set of minimally invasive sensors are placed on the patient’s face, without interfering with function. A high-precision, high-frequency (120 Hz) infrared optical camera records the
patient’s movements and integrates them into the patient’s intra-oral scans (Fig. 6).5,6 For the first time, this enables us to see what is happening in patients’ mouths.
The software design is intended to optimise the user experience. The practitioner can manipulate the 3D models on the computer’s touch screen. The acquisition interface is divided into three main panels (Fig. 7):
- On the left are all the functions for interacting with the 3D models of the patient. The features are divided into three modules: ACCESS, ADVANCED and AESTHETIC.
- In the middle are the recorded movements and the replay
functions for for analysis by the dentist after the patient leaves. - On the right the trajectories of three anatomical points (right condyle, left condyle and sub-nasal point) in the three planes of space.
The repeatability of MODJAW recordings has been found to be good to excellent.7 It is important to note that the precision of the system directly depends on the input data (3D models from intra-oral scanners, CBCT scan and facial scan).

Fig. 4: MODJAW Tech in Motion system. Fig. 5: MODJAW hardware. Fig. 6: MODJAW trackers.
Creation of a dynamic digital twin
Digital twins are digital prototypes or replicas of the patient. Real-time jaw motion of the patient adds a layer of dynamic information, essential for offering a personalised treatment.8
The data collection is begun by taking intra-oral scans to obtain the 3D models of the actual maxillary and mandibular situation in static occlusion (maximal intercuspal position). In addition, 2D photographs and a facial scan capture extra-oral and intra-oral information for documentation and education and act as a reference for before and after treatment comparisons.1
A CBCT scan is performed to gain 3D visualisation of the craniofacial structures for examination and treatment initiation (Fig. 8). The benefits of a CBCT scan in the oral and maxillofacial surgery field include diagnosis of bone pathology and developmental anomalies. In implantology, a CBCT scan permits the area surrounding the future implant to be investigated, along with evaluation of the height, width and quality of the alveolar bone and awareness of the surrounding anatomical structures.2
All the data mentioned is collected and imported into the MODJAW software to record the mandibular kinematics of the patient and to get closer to creating a dynamic digital twin (Figs. 9 & 10).

Fig. 7: MODJAW software. Fig. 8: Facial scan of the patient, matched with the 3D models and the CBCT scan. Fig. 9: Segmented CBCT scan. Fig. 10: Motion applied to the segmented CBCT scan.
Aesthetic Evaluation
Numerous software programs (e.g. DSD, Smilecloud and SmileFy) are available to obtain an aesthetic preview of the prosthetic project for communication with the patient and promotion of acceptance of the proposed therapy.9–11 The aesthetic evaluation and planning in this case were performed on the Smilecloud platform. It offers adaptative libraries, providing hundreds of possible designs.
The choice is made according to parameters such as the smile line, the position of the lips, the smile and the bipupillary line (Fig. 11). Once the aesthetic evaluation has been done and validated, the chosen library is exported as a 3D model to the laboratory (Fig. 12).
Functional evaluation
The following records were registered with MODJAW Tech in Motion:
– open and close;
– protrusion;
– left and right laterotrusion;
– centric relation;
– speech; and
– mastication.
After the first step of recording has been done, a dynamic evaluation is conducted using the MODJAW software. It helps to identify two pieces of information: the mandibular position and the functional envelope of the patient can be preserved, as described later.
The mandibular position was evaluated by recording the centric relation. The patient was guided into centric relation using the bimanual guided Dawson technique, to record open and close movements of small amplitude so that the condyles remained in pure rotation (Fig. 13).12 The trajectories of the inter-incisal point in a frontal and sagittal plane and the left and right condyle in the sagittal plane showed a
reproducible CR that coincide with maximal intercuspation position (MIP).
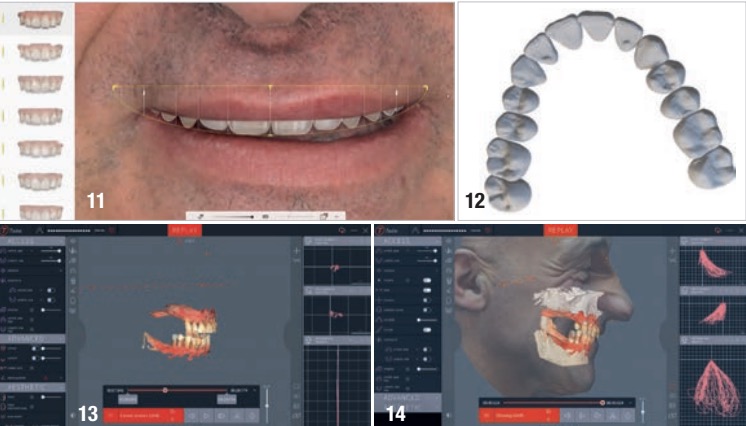
of the tooth library. Fig. 13: Analysis of the patient’s centric relation. Fig. 14:
Analysis of the patient’s jaw motion: sharp and symmetric masticatory
pattern and the teeth still guiding.
The analysis of the tracing of the inter-incisal point in the frontal and sagittal planes and the left and right condyles in the sagittal plane showed a reproducible centric relation that coincided with maximal intercuspal position.
The second evaluation checked the patient’s envelope of function by analysing the border limit movements (open/close, protrusion and laterotrusion) and the masticatory pattern. It showed a good guidance and a perfect correlation between the interincisal point path and the left/right condylar path. The analysis of the mastication showed a good masticatory pattern, very well guided by the residual teeth and a sharp and symmetric masticatory pattern on the left and right condylar trajectories (Fig. 14).
Therefore, it was decided to keep the current mandibular position and the functional envelop of the patient for the prosthetics design. In order to do that in a digital workflow, all the static and dynamic patient data was exported from MODJAW as standard files and imported into exocad.
Treatment planning: Prosthetic and implant planning
MODJAW data provides the dental technician with the following necessary information to design in exocad:
– the mandibular position in the three spatial planes;
– the patient’s jaw motion to adapt the occlusal morphology and the occlusal plane while respecting the functional curves of Spee and Wilson;
– the border limit movement to adjust the anterior guidance according to the protrusion and laterotrusion recorded; and
– the masticatory movements to adjust the cusps of the posterior reconstruction.
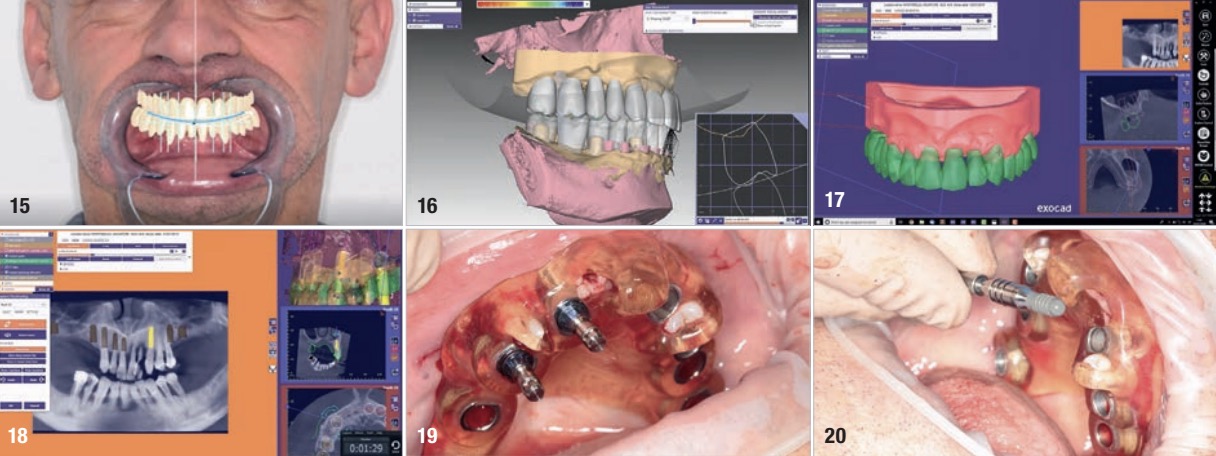
With the collection of this information, an optimal and balanced prosthetic design according to the chosen occlusal concept can be achieved.13 The prosthetic project is called a 4D wax-up because of the use of the dynamic movement in the design process (Figs. 15 & 16).4,14
Once this 4D wax-up has been created and validated, it becomes the reference that will guide each step of the implant planning. Thanks to the superimposition of the 4D wax-up on the CBCT scan in exoplan (exocad), the implants are virtually positioned in an ideal position (Figs. 17 & 18). While the implant placement was planned, a virtual extraction of some teeth on the initial model allowed the design of
several guides. For each arch, two guides were created. The first guide had mixed mucosal and dental support. The idea was to keep the necessary teeth to maintain the guide and place the first implants, because a guide with dental and mucosal support offers more precision than one with only mucosal support (owing to possible mobility).15 A second guide was designed on a fully extracted model to allow the surgeon total access to the last implant site.
By exporting the 4D wax-up and the position of the implants, the dental technician has the necessary information to create the temporary prosthesis, including aesthetic and functional recommendations to guide the healing process in the best way. The surgeon receives the surgical protocol from the planning, as well as the surgical guide and the prosthesis ready to be screwed in.
Surgical phase and immediate loading
After anaesthesia, the first teeth were extracted. The first guide was used to place the first implants in the mandible and maxilla (Fig. 19). After that, the residual teeth were extracted, and the second guide was fixed on the implants already in place to continue placement of the other implants.
For the maxilla, bone augmentation was not planned. There was still the possibility of managing implant placement with osteotomy preparation and crestal access according to the Summers’ technique (Fig. 20).16,17 The sleeves of the surgical guide led the osteotomy preparation in sites #16 and 26.18 After all the implants had been placed, the Variobase (Straumann) and temporary abutments were screwed in.
The prostheses had already been milled ahead of surgery (Figs. 21 & 22). On the maxilla, a support on the palate allowed us to stabilise the prosthesis and connect it in the correct situation. We then injected composite to attach it to the temporary abutments. For the mandible, the prosthesis was attached in the same manner in occlusion (Fig. 23). Everything was then unscrewed again and polished and the occlusion checked (Figs. 24 & 25).


Discussion
In this type of situation, multiple parameters need to be mastered, including bone management, aesthetic evaluation, functional evaluation and psychology. With new digital tools, the dentist is able to evaluate the patient and collect all the data, static and dynamic. Additionally, the dentist is able to delegate a part of the work to the laboratory by fully virtualising the patient and sharing the digital twin with the dental technician.
This clinical case highlights how the practitioner can gain a comprehensive idea of the initial situation both aesthetically and functionally and understand the compensation mechanism of occlusion and the impact on the mandibular position and movements. Once the initial evaluation has been done, jaw-motion records allow the conservation of the functional initial situation in the prosthetic project.
Motion data is very valuable in a situation of immediate loading, as jaw motion is partially driven by proprioception that programmes muscular contraction and is in the muscle memory.
After the surgery, mandibular movement will only be driven by muscular exteroception recorded on the initial situation. Thus, when the designed prostheses including the initial functional movement are placed, the entire stomatognathic system will not encounter any obstacle and integration will be smoother.
Conclusion
The new tools in digital dentistry redefine traditional protocols. They keep improving the predictability and quality of treatment while simplifying the processes. Managing the dynamic occlusion of implant restorations in a completely digital workflow is a reality with MODJAW Tech in Motion. The practitioner is able to evaluate the mandibular position and the dynamic motion of the patient and to integrate a new set of data in the prosthetic project to create a static and dynamic occlusion.
Note: This article originally appeared in digital – international magazine of digital dentistry Vol. 4, Issue 1/2023, and is republished here with permission from Dental Tribune International GmbH.
About
Dr Maxime Jaisson holds a master’s degree in biomechanics from the University of Reims
Champagne-Ardenne in France, a university diploma in applied facial prosthetics and a doctorate in
odontological sciences. He is a dental surgeon and a co-founder of MODJAW.
Dr Marion Paris is a dental surgeon specialised in oral surgery. She is a clinical director at Ardentis dental and orthodontic clinics and was formerly a university lecturer and hospital practitioner at the
then Paris Diderot University (now Université Paris Cité) in France.
Dr Ouassim Salmi holds a master’s degree in digital dentistry from Université Paris Cité in France. He is a dental surgeon and a clinical manager at MODJAW.
References
1. Wismeijer D, Joda T, Flügge T, Fokas G, Tahmaseb A, Bechelli D, Bohner L, Bornstein M, Burgoyne A, Caram S, Carmichael R, Chen CY, Coucke W, Derksen W, Donos N, El Kholy K, Evans C, Fehmer V, Fickl S, Fragola G, Gimenez Gonzales B, Gholami H, Hashim D, Hui Y, Kökat A, Vazouras K, Kühl S, Lanis A, Leesungbok R, van der Meer J, Liu Z, Sato T, De Souza A, Scarfe WC, Tosta M, van Zyl P, Vach K, Vaughn V, Vucetic M, Wang P, Wen B, Wu V. Group 5 ITI consensus report: digital technologies. Clin Oral Implants Res. 2018 Oct;29 Suppl 16:436–42. doi: 10.1111/clr.13309.
2. Kazis H, Kazis AJ. Complete mouth rehabilitation through fixed partial denture prosthodontics. J Prosthet Dent. 1960 Mar–Apr;10(2):296–303. doi: 10.1016/0022-3913(60)90057-3.
3. Tiwari B, Ladha K, Lalit A, Dwarakananda Naik B. Occlusal concepts in full mouth rehabilitation: an overview. J Indian Prosthodont Soc. 2014 Dec;14(4):344–51. doi: 10.1007/s13191-014-0374-y.
4. Felenc S. La 4D et le flux de travail numérique: enjeux et applications cliniques. QDRP. 2020 Dec;14(4):353.
5. Felenc S, Jaisson M. Apport du digital aux choix fonctionnels et esthétiques: l’intérêt de la dentisterie 4D. QDRP. 2018 Nov;12(4):335–46.
6. Jaisson M, Felenc S. Comprendre la CFAO 4D. L’Information Dentaire. 2018 Jan 18 [cited 2023 Feb 20]. Available from: https://www.information-dentaire.fr/formations/comprendre-la-cfao-4d/.
7. Bapelle M, Dubromez J, Savoldelli C, Tillier Y, Ehrmann E. Modjaw® device: analysis of mandibular kinematics recorded for a group of asymptomatic subjects. Cranio. 2021 Nov 6:1–7. doi: 10.1080/08869634.2021.2000790.
8. Sun T, He X, Song X, Shu L, Li Z. The digital twin in medicine: a key to the future of healthcare? Front Med (Lausanne). 2022 Jul 14;9:907066. doi: 10.3389/fmed.2022.907066.
9. Zimmermann M, Mehl A. Virtual smile design systems: a current review. Int J Comput Dent. 2015;18(4):303–17. English, German.
10. Cervino G, Fiorillo L, Arzukanyan AV, Spagnuolo G, Cicciù M. Dental restorative digital workflow: digital smile design from aesthetic to function. Dent J (Basel). 2019 Mar 28;7(2):30. doi: 10.3390/dj7020030.
11. Coachman C, Calamita MA, Sesma N. Dynamic documentation of the smile and the 2D/3D digital smile design process. Int J Periodontics Restorative Dent. 2017 Mar/Apr;37(2):183–93. doi: 10.11607/prd.2911.
12. Orthlieb JD, Ré JP, Perez C, Darmouni L, Mantout B, Gossin G, Giraudeau A. La relation centrée myostabilisée: un concept simple, physiologique et consensuel. Cah Prothese. 2008 Mar;141:13–21.
13. Pascual D. Réhabilitation d’arcade complète avec mise en charge immédiate d’une prothèse d’usage à armature métallique dans la même séance. TITANE. 2019.
14. Rabiey A. Flux numérique: de la mise en charge immédiate à la prothèse d’usage en prothèse complète implanto portée. AOnews. 2021 Nov [cited 2023 Feb 20]. Available from: http://www.aonews-lemag.fr/numerique-ahmed-rabiey-aonews/.
15. Ozan O, Turkyilmaz I, Ersoy AE, McGlumphy EA, Rosenstiel SF. Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant placement. J Oral Maxillofac Surg. 2009 Feb;67(2):394–401. doi: 10.1016/j.joms.2008.09.033.
16. Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium. 1994 Feb;15(2):152, 154–6, 158 passim; quiz 162.
17. Summers RB. The osteotome technique: part 3—less invasive methods of elevating the sinus floor. Compendium. 1994 Jun;15(6):698, 700, 702–4 passim; quiz 710.
18. Paris M, Chaux-Bodard AG, Gourmet R, Fortin T. Guided implant surgery on oral cancer patients: in vitro study. Int J Comput Assist Radiol Surg. 2011 Jan;6(1):135–42. doi: 10.1007/s11548-010-0490-z.